When to operate?
The thyroid is an endocrine gland located in front of the neck, it has the function of managing the growth and energy of the human body. It can be affected in its morphology (increase in size, benign or malignant tumor) or its endocrine function: normal (euthyroidism), decreased (hypothyroidism) or increased (hyperthyroidism).
Thyroid surgery is part of a multidisciplinary management involving endocrinologists, radiologists, surgeons and other specialists.
After a possible preparation for the operation, a thyroidectomy should be performed in the following situations:
1) Goiter: increased thyroid volume due to nodules or cysts
2) A thyroid nodule: "ball" that may correspond to a benign (most common) tumour or cancer (more rarely).
3) Hyperthyroidism due to hyperfunction of the entire gland (Basedow's disease) or a "toxic" nodule located in a part of the thyroid.
4) The recurrence of a disease after a previous partial thyroid operation.
What type of operation:
All operations are carried out with complete narcose.
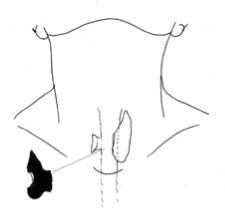
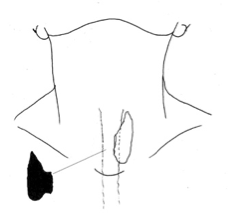
The thyroid had an "H" form, with 2 lobes connected by an isthma. Depending on the disease, the following operations are proposed:
Lobo-Isthmectomie sub-totale
What are the risks during and after the operation:
1) Recurrent nerve (also called lower laryngeal nerve):
It is a nerve that passes on either side of the neck behind the thyroid. He is still wanted, identified and protected during the operation. It controls the vocal cords, whose role is to be able to speak and close access to the lung to avoid choking when eating. A blockage of the nerve impulse (whether the nerve is intact or injured) thus causing a weak or hoarse voice is a rare phenomenon (about 5-10% of operations), not predictable and especially temporary with a recovery in a few days or weeks.
2) Parathyroids
These are 4 glands located in the neck around the thyroid, their role is to regulate calcium metabolism. A single healthy gland is enough to ensure a normal function. During thyroid surgery, the parathyroid glands may be endangered due to their close proximity to the thyroid. Symptoms (sensation of ants on the hands and face, cramps) could occur in 5-10% of cases. Treatment is a temporary calcium substitution.
Benefits of surgery and post-operative follow-up:
The purpose of the operation is to remove a voluminous goiter, one or nodules suspected of cancer or a thyroid gland that works too much. These operations were proposed because another treatment was not possible or failed.
After a thyroidectomy, a thyroid hormone substitution (1 tablet per day) must be introduced within a few days and requires monitoring by taking blood samples once or twice a year. The follow-up is provided by your treating physician or an endocrinologist. In the case of thyroid cancer, a specialist endocrinologist will give you additional information, as to whether or not to provide another complementary treatment.